Partial-hand amputations
Severed fingers and other partial-hand amputations are incredibly serious injuries requiring patients to undergo a long and onerous road to recovery
Oh, how we take our hands for granted. We use them in virtually every single activity we engage in throughout the day, without paying much attention. They grasp, grip, pinch, push, pull, manipulate, etc. We use them to push ourselves out of bed, brush our teeth, bathe, dress, prepare food, feed ourselves, drive to work, use our phones, write, type, open doors, refrigerators and cabinets, open jars, remove items from our pockets, hand over money or a credit card, bring in the groceries, scratch an itch, hold a loved one’s hand, break a fall, and so much more.
Violate the golden rule for just a few moments and imagine what it would be like to have the use of one of your hands permanently compromised. Spend a day particularly noticing how often and in how many different ways you use your hands, and what it might be like if one of your hands was not fully functional. Then think about the feelings you would experience each time you struggled or looked at your hand and noticed the deformity, or the potential embarrassment of having others notice. Partial- hand amputations are permanently life altering.
There are approximately 45,000 traumatic finger amputations each year in the United States (see Conn J, Annest J, Ryan G. Non-work-related finger amputations in the United States, 2001-2002. Ann Emerg Med. 2005;45:630-5; McCall B, Horwitz I. An assessment and quantification of the rates, costs, and risk factors of occupational amputations: analysis of Kentucky workers’ compensation claims, 1994-2003. Am J Ind Med. 2006; 49:1031-8; Boyle D, Parker D, Larson C, Pessoa-Brandao L. Nature, incidence, and cause of work-related amputations in Minnesota. Am J Ind Med. 2000; 37:542-50; Centers for Disease Control and Prevention; [Accessed August 1, 2014]. www.2a.cdc.gov/risqs/) – many being personal injuries suffered due to the fault of another.
As attorneys we owe it to these clients to understand how their lives have been impacted by such serious injuries, and to understand what it takes to restore as much of what they have lost, as possible.
Products liability
For the last decade, a large percentage of my practice has been dedicated to representing plaintiffs in product-liability cases arising out of workplace injuries involving industrial machinery, which unfortunately presents many hazards to its users, particularly to their hands. I have represented plaintiffs who have suffered partial-hand amputations (through the fingers, thumb, and/or transmetacarpal/palm region of the hand) while using table saws, band saws, vegetable slicers, pillow- filling machines, juicers, and punch presses (to name just a few), which were not equipped with adequate safety devices. Depending on the type of equipment, and its component parts, whether it be rollers with pinch points, rotating knives, die presses, or simple gears, a user can suffer any number of injuries to their hands while using such equipment, such as crushing injuries, tearing injuries, avulsion injuries or severing injuries, resulting in traumatic amputations.
Each type of partial- hand amputation, and the level of the hand at which it occurs, presents complicated medical issues for the victim, and varying methods of treatment and rehabilitation.
Surgery and other treatment
Surgeries addressing such injuries include replantation, revision, ray resection, and reconstruction, to name only some. Of course, the ultimate goal of these surgeries is to preserve length of the residual limbs and restore function and/or improve cosmesis (aesthetics). Further, often hyperbaric oxygen treatment is necessary to increase tissue oxygen concentration in order for the amputation to heal properly, as is tissue grafting (transplanting skin, tendons and/or blood vessels, from one body area to be applied to the wound in another area).
Replantation
Replantation is the surgical reattachment of a finger or fingers. Such surgeries can be successful if the digits, tissue and vascular structures are viable and in good condition (unlikely in the case of crush injuries), if the digits are properly preserved, and the surgery is performed in short order (usually within six hours of the amputation). The procedure involves debridement (removal of damaged tissue); revision (shortening) of bone ends, muscles, tendons, nerves, arteries, and veins; rejoining and fixation of bones with pins, wires, plates and/or screws; skin, tissue and/or blood vessel grafting; repair of tendons, nerves and veins; and wound closure. Replanted digits generally will be stiff, with approximately a 50% reduction in total motion.
Ray resection
Ray resection involves amputation of an entire digit and may be indicated when there is ischemic necrosis (death of tissue caused by deprivation of blood supply) of the metacarpal, severe dysfunction of the proximal interphalangeal joint, or amputations at the proximal phalanx. Such conditions may cause pain and stiffness, affecting the dexterity and function of other viable digits. Ray resection in such cases may be performed to improve the overall function of the hand. In certain cases, ray resection can be indicated to improve cosmesis.
Revision
Revision surgery is surgery to further shorten the bone and surrounding structures beyond the level of the original amputation. It may be necessary for a variety of reasons, including, but not limited to, poor healing from the original amputation, to address pain, extra skin, skin break down, painful scars, bones beginning to protrude through the skin, etc. Additionally, revision surgeries may be performed to aid in the fitting of prosthetic devices.
Reconstruction
Reconstructive surgeries may include transplantation of digits (such as toe to thumb, or little finger to index finger), grafting, or local flap reconstruction (using the remaining intact skin and blood supply to cover the residual bone).
Surgeries may also include neurectomies (the surgical removal of all or part of a nerve) to address pain, targeted muscle reinnervation (a nerve transfer technique where proximal stumps of the transected major peripheral nerves are transferred to recipient redundant motor nerves within adjacent muscles of the amputated limb) and/or surgery to address syndactyly (abnormalities in the way the fingers are connected and/or deformities in the webbing between the fingers). (See Cheesborough JE, Smith LH, Kuiken TA, et al., Targeted muscle reinnervation and advanced prosthetic arms, Semin Plast Surg. 2015; 29:62-72; Cheesborough JE, Souza JM, Dumanian GA, et al., Targeted muscle reinnervation in the initial management of traumatic upper extremity amputation injury, Hand (N Y). 2014; 9:253-257; Valerio IL, Dumanian GA, Jordan SW, et al., Preemptive treatment of phantom and residual limb pain with targeted muscle reinnervation at the time of major limb amputation, J Am Coll Surg. 2019; 228:217-226; Dumanian GA, Potter BK, Mioton LM, et al., Targeted muscle reinnervation treats neuroma and phantom pain in major limb amputees: A randomized clinical trial. Ann Surg. 2019; 270:238-246; Alexander JH, Jordan SW, West JM, et al., Targeted muscle reinnervation in oncologic amputees: Early experience of a novel institutional protocol. J Surg Oncol. 2019; 120:348-358.)
Most often, victims of amputation injuries will have to undergo a series of surgeries to restore function and cosmesis, over the course of many years. To say the least, partial-hand amputations are incredibly serious injuries requiring patients to undergo a long and onerous road to recovery. In addition to these painful and protracted surgical interventions, partial-hand amputees undergo various forms of physical and occupational therapy in an attempt to restore as much function to the hand as possible. Further, ongoing pain management, in the form of opioid pain medication and/or alternative treatments such as acupuncture, chiropractic care, massage therapy, transcutaneous electrical nerve stimulation (TENS) and implantable peripheral nerve stimulators, may be indicated to treat amputation-related pain.
Residual symptoms
Partial-hand amputees may have a variety of symptoms such as residual limb pain; phantom pain (the sensation of feeling pain in a limb that is no longer present, which can mimic the feeling of the limb being crushed, and/or sometimes described as “lightning bolts” or “zingers”); nerve pain or neuromas resulting from the ends of the amputated nerves forming endings of axons and scar to which pressure being applied can result in very sharp pain; cramping; increased sensitivity; intolerance to cold; chronic sores due to fragile skin at the amputation site; severe infection (i.e., osteomyelitis) when the bone is close to the surface; scarring; reduced range of motion, motor strength and grip strength, making manipulative tasks extremely difficult; pain due to overuse of the sound limb, including degenerative and repetitive overuse conditions which arise over time; postural scoliosis resulting from tightening of muscles when the patient repetitively holds the arm close to the chest in an effort to guard or protect the injured hand; mental health conditions such as PTSD, depression, avoidance and embarrassment, anxiety about reinjury; as well as impact on cognitive abilities such as focus and concentration. In most instances, psychological care is required.
Prosthetics and orthotics
With the goal of restoring function and cosmesis, a wide variety of prosthetics (devices to replace a limb) and orthotics (devices to enhance the function of a limb) are available for partial hand amputations. The types of such devices available depend largely on the length of the residual limb and the goal of the patient. There are passive devices, mainly used to improve the aesthetic appearance of the hand, as well as active or functional devices used to restore the ability to perform various activities unable to be performed due to the amputation. Patients work with specialists in the field including orthopedists and prosthetists to obtain the appropriate devices, accordingly.
Passive prosthetics
Passive prosthetics for partial-hand amputations may include custom silicone fingers designed to lengthen the digits and replicate the amputated fingers as closely as possible. They also protect the sensitive areas of the amputation site. Such silicone digits can be made to mirror the digits on the uninjured hand. Great skill is employed to match the color and skin tone to create a seamless appearance. Often, multiple sets may be required, such as in the case of skin tone which greatly differs with the seasons. As the tone of the hand’s skin may become tanner in the summer, an alternative set of darker silicone fingers can be made to be worn during such times, to make the presence of the prosthetics less obvious.
Passive prosthetics, though may have some limited use in improving function, generally are unable to perform grasping or releasing activity, as the fingers generally do not bend, and do not necessarily have the same pinch force as some of their mechanical counterparts. However, silicone fingers may help in activities such as pushing, pulling, typing or picking up objects off a table, as silicone has friction characteristics that help with such functions. Other passive devices, which enhance function to some degree, may include those with multi-positional finger joints, or ratcheting fingers that can be made to flex at the joints. Thumb prosthetics are also available where the thumb is locked in a fixed position to assist with grasping functions.
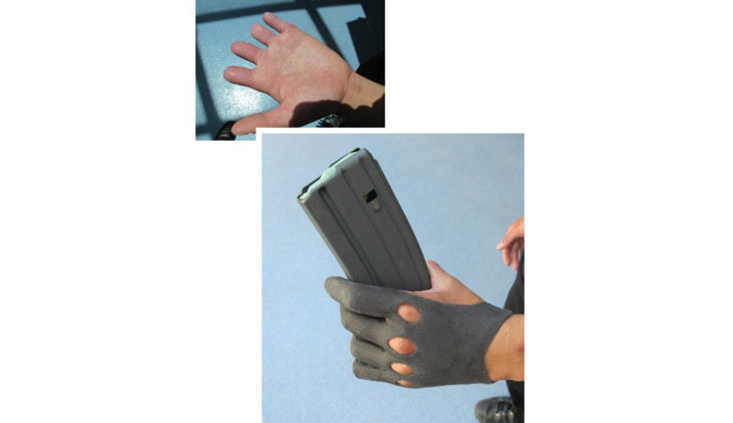
Because custom silicone prostheses can be torn, stained or otherwise damaged during use in various activities, prosthetists will often recommend a more durable and thicker silicone utility glove for use during such activities, which may or may not be custom painted. Such gloves may help, in limited fashion, improve functions such as grasping as well.
Body-powered prosthetics
There are a wide variety of partial hand prostheses which are body powered, whereby they are directly controlled by the patient’s wrist or other portions of the hand and provide functional benefits by way of increased force and dexterity. They are, in essence, a mechanical extension of the hand, which is 3D-printed in titanium, brass and/or stainless steel, and may include heavy-duty ratcheting mechanisms.
They help to improve range of motion, such as flexion and extension, enhance the ability to grasp objects, to lift and carry heavier objects and, like passive prosthetics, also extend digit length. Typically, such devices are operated by way of a harness and cables.
Such prosthetics may include a terminal device such as a hook or a hand. Body-powered prostheses are also generally more durable than passive prosthetics such as custom silicone fingers, making them useful for work in certain environments that are dirty, dusty, wet, hot, etc. They are available through manufacturers such as Naked Prosthetics, Point Designs and Partial Hand Solutions, LLC. Patients with body-powered prosthetics, however, may experience symptoms from overuse or repetitive stress injuries in adjacent body parts that are exerted in the use of body-powered prosthetics.
Externally powered/electronic prosthetics
In some cases, partial-hand amputations, depending on the level at which they occur, can be aided by the use of externally powered/electronic multi-articulating prosthetics. Such devices currently include the Vincent hand by Vincent Systems, the iDigit by Ossur, and the sDigit out of Italy. They are myoelectric devices, which include sensors on the back of the hand and forearm that pick up on signals sent by the brain to these parts of the hand and consequently send signals to the electronic digits that have small motors in them.
These devices help the patient to flex his/her fingers and exert varying degrees of power, which provides assistance in grabbing and stabilizing items. Generally, these are currently used where amputations are at the metacarpophalangeal joint, and there remains a portion of the proximal phalynx, however it is expected that with the advancement of technology, such devices will, within the next decade, be available to partial hand amputees where the level of the amputation is not as proximal as is currently required for the use of electronic prosthetics to be indicated.
With all such prosthetic devices, there are annual maintenance costs, costs of replacement/repair of minor and major componentry, as well as the necessity of complete replacement of the prosthesis, which is generally every two to three years for silicone prostheses and every three to five years with body-powered and electronic prostheses.
Working with experts
It is essential, when representing clients with partial-hand amputations, to retain experienced experts in amputation injuries, such as orthopedists and hand surgeons as well as prosthetists, not only to be able to testify with clarity regarding the nature of the injuries sustained, the medical treatment received, and the client’s prognosis, but to opine on the necessity of future medical care and prosthetics, as well as the cost thereof.
An expert psychologist is also recommended to testify regarding mental health conditions that the client may be experiencing as a result of the injuries sustained and impact on the client’s life, as well as the need for future psychological care.
A physiatrist should also be retained to create a comprehensive life care plan consisting of not only the future medical care, and recommended prosthetic devices, but to include the cost of any other assistance that partial hand amputees will typically require due to inabilities to perform certain activities of daily living (ADL).
Additionally, because the loss of function of one hand, particularly if it is the dominant hand that has been injured, can have a profound impact on the ability of the client to earn a living, a vocational- rehabilitation expert is useful to substantiate the client’s loss of earnings/earning capacity claims. Finally, a forensic economist should be employed to perform the necessary calculation of such economic damages and reduce them to present value.
Understanding clients to best advocate on their behalf
At the beginning of this article, I asked the reader to violate the golden rule and try to imagine what it might be like to suffer an amputation and lose the function of a hand. Obviously, it would be impermissible to ask a jury to do the same. However, an attorney can still convey the profound impact of a partial-hand amputation to the jury if he/she takes the time to understand the plaintiff on a deeper level than simply asking questions.
As with any serious injury, it is extremely helpful to spend a day shadowing the client. Observing the difficulties that a person with such an amputation encounters throughout the day offers a glimpse into the impact such an injury has on one’s life. To be there with the client as they struggle with limitations in their functionality, the physical sensations they experience throughout the day, and mental anguish and frustration that is inherent in the life of individuals who have had the misfortune of suffering this type of injury, is the best primer for the lawyer to be able to understand and articulate, and be able to elicit testimony from the client, about the true human damages that are entailed when such injuries occur. Interviewing family members, friends and co-workers, may also offer insight into the client’s struggle with their injuries, or the way in which they persevere in the face of their limitations. Further, Day-in-the-Life videos can be a useful tool to present to the jury the daily challenges endured by such clients.
Conclusion
Partial-hand amputations are incredibly complex injuries. Much time should be spent understanding their nature, the impact they have on the client’s life, and the future medical care and prosthetics that will be necessary to help the client function and cope with limitations, as best as possible. Most of all, compassion and empathy for your clients will help in navigating them through the legal process on the road to civil justice.
Jeffrey A. Rudman

Jeffrey A. Rudman is the President of the Consumers Attorneys Association of Los Angeles (CAALA) and the Principal of The Rudman Law Firm, APC, a boutique Martindale-Hubbell AV rated Plaintiff’s law firm handling catastrophic injury and wrongful death cases. Jeff has served on the CAALA Board since 2008, and has served as a chair of CAALA’s Membership Committee, Las Vegas Convention, and Education Committee. He is also credited with the creation of CAALA’s Online Document Bank.


Copyright ©
2026
by the author.
For reprint permission, contact the publisher: Advocate Magazine